Post by Allen on Jul 8, 2014 9:19:04 GMT -8
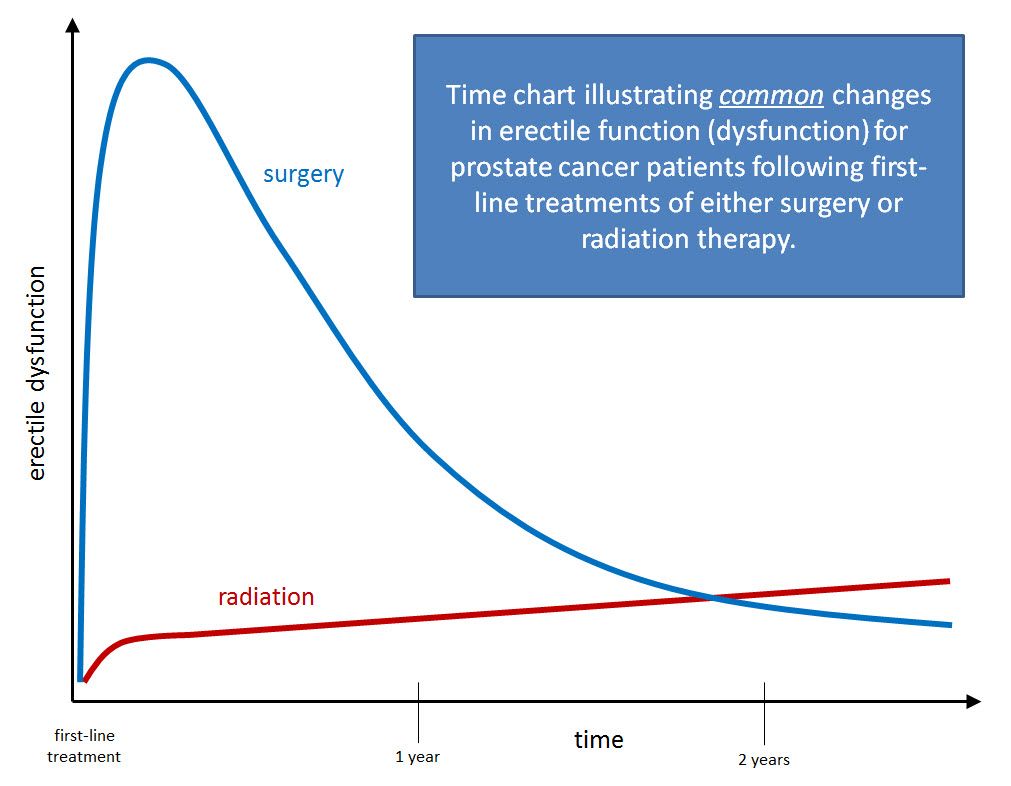
One of the most important things we patients want to know about any treatment is what kind of potency we can expect afterwards.
While there is at least some consensus on the use of CTCAE4.0 to grade urinary and rectal morbidity, there seems to be no consensus on sexual dysfunction. It is reported in a wide variety of different, non-comparable ways, if it is reported at all.
Several definitions are used in research: IIEF-6, EPIC-sexual status score, erection sufficient for intercourse, and actual intercourse in the last month, whether erection aids are needed or helpful. Often, results are given among men who were previously potent or high scoring only. Others report return to baseline function, where “return” may be defined as anything from within 1 point on IIEF-6 to anything within the population standard deviation.
From the patient’s point of view, we would love to have a nomogram that could predict our probability of potency for any given treatment.
Because so many of us rely on the Sanda study (attached), perhaps that should set the standard. However, there is a problem in the way they use baseline EPIC scores and age in their predictive model. Sexual Function after PC therapy.pdf (391.83 KB)
Here’s the multiple linear regression model they found for surgery (Table 1):
Likelihood of functional erections= -2.96 + .45*EPICSCORE - .56*AGE + …
(Age & EPIC score were categorized in multiples of 10)
The problem is that EPIC score is not independent of age - it is a function of age, especially in the age group studied. This violates a basic assumption of the model. It seems the problem of covariance is easily fixed by using an age-adjusted EPIC score (much as we use inflation-adjusted constant dollars in economic analyses). U of Michigan must have a validated file of EPIC scores by age for a random sample of healthy men. Those scores, expressed as a percent, can become an indexing factor that will be divided into each respondent’s EPIC score according to his age.
The Sanda study only looked at potency 2 years after treatment, so the effect of aging was negligible. This is more than just a technicality. As we measure potency after treatment for say 5 or 10 years, we want to separate treatment effects from age effects.
So a revised model might look something like:
Likelihood of functional erections at time t = a + b x EPICSCORE (age adjusted at baseline) + c x AGE + d x TIMESINCETREATMENT + …
Alternatively, we could find a predicted EPIC score at a future time:
EPICSCORE (age adjusted at time t)= e + f x EPICSCORE (age adjusted at baseline) + g x AGE + h x TIMESINCETREATMENT + …
Other independent categorical variables will depend on the thoroughness of the records and may include: married or has sex partner, ED meds, cardiovascular disease, diabetes, neuropathy, beta-blockers, depression, substance abuse, obesity, smoking, hypogonadism, and use of ADT. These may explain some of the variance in the likelihood of potency or predicted sex EPIC score as long as they held for a given patient throughout the study period. However, if any of these categorical variables changed during the observation period (e.g., the man got a new young girlfriend or gave up smoking after treatment) they will be confounding.
So my questions are:
1. How can we get medical researchers to arrive at a consensus about this?
2. How can we develop a nomogram that will predict potency for each treatment type?
While there is at least some consensus on the use of CTCAE4.0 to grade urinary and rectal morbidity, there seems to be no consensus on sexual dysfunction. It is reported in a wide variety of different, non-comparable ways, if it is reported at all.
Several definitions are used in research: IIEF-6, EPIC-sexual status score, erection sufficient for intercourse, and actual intercourse in the last month, whether erection aids are needed or helpful. Often, results are given among men who were previously potent or high scoring only. Others report return to baseline function, where “return” may be defined as anything from within 1 point on IIEF-6 to anything within the population standard deviation.
From the patient’s point of view, we would love to have a nomogram that could predict our probability of potency for any given treatment.
Because so many of us rely on the Sanda study (attached), perhaps that should set the standard. However, there is a problem in the way they use baseline EPIC scores and age in their predictive model. Sexual Function after PC therapy.pdf (391.83 KB)
Here’s the multiple linear regression model they found for surgery (Table 1):
Likelihood of functional erections= -2.96 + .45*EPICSCORE - .56*AGE + …
(Age & EPIC score were categorized in multiples of 10)
The problem is that EPIC score is not independent of age - it is a function of age, especially in the age group studied. This violates a basic assumption of the model. It seems the problem of covariance is easily fixed by using an age-adjusted EPIC score (much as we use inflation-adjusted constant dollars in economic analyses). U of Michigan must have a validated file of EPIC scores by age for a random sample of healthy men. Those scores, expressed as a percent, can become an indexing factor that will be divided into each respondent’s EPIC score according to his age.
The Sanda study only looked at potency 2 years after treatment, so the effect of aging was negligible. This is more than just a technicality. As we measure potency after treatment for say 5 or 10 years, we want to separate treatment effects from age effects.
So a revised model might look something like:
Likelihood of functional erections at time t = a + b x EPICSCORE (age adjusted at baseline) + c x AGE + d x TIMESINCETREATMENT + …
Alternatively, we could find a predicted EPIC score at a future time:
EPICSCORE (age adjusted at time t)= e + f x EPICSCORE (age adjusted at baseline) + g x AGE + h x TIMESINCETREATMENT + …
Other independent categorical variables will depend on the thoroughness of the records and may include: married or has sex partner, ED meds, cardiovascular disease, diabetes, neuropathy, beta-blockers, depression, substance abuse, obesity, smoking, hypogonadism, and use of ADT. These may explain some of the variance in the likelihood of potency or predicted sex EPIC score as long as they held for a given patient throughout the study period. However, if any of these categorical variables changed during the observation period (e.g., the man got a new young girlfriend or gave up smoking after treatment) they will be confounding.
So my questions are:
1. How can we get medical researchers to arrive at a consensus about this?
2. How can we develop a nomogram that will predict potency for each treatment type?